2.2.1 Private Consumption
Introduction
Private consumption is the value of goods and services consumed by individuals, households, or NPISHs that are acquired through the private sector. We assume that all consumption can be assigned to individuals. This assumes away pure public goods, economies of scale, and other important features of consumption and production.
Private consumption is typically allocated to individuals based on household surveys. The methods described here assume the availability of one or more household surveys which include detailed expenditure data for the household and the number and age of all household members. Ideally the surveys are nationally representative.
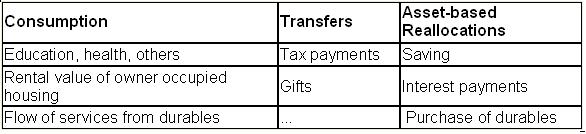
Household expenditure surveys usually include all household expenditures or outflows. Although only consumption expenditures are needed to estimate consumption age profiles, other outflows are used to estimate other NTA components. Thus, it is useful to classify all household expenditures or outflows during the year as falling into one of three categories - consumption, transfers, or asset-based reallocations:
NTA methodology distinguishes three components of private consumption: education, health, and other consumption. Education and health are estimated separately because they vary substantially by age.
Private education consumption includes tuition, books and fees, school supplies for all school levels including pre-school and tutoring expenses. The exact definition will vary depending on data availability. In Taiwan, for example, reference materials and self-improvement classes (art classes, music classes, etc.) are also included.
Private health consumption includes out-of-pocket health expenditure and reimbursement to health providers by private health insurance companies. If firms provide medical services directly to their employees and their dependents, the value of these services are also included in private health consumption. It is important to note that there are differences between NIPA and NTA, and between NIPA and National Health Account (NHA).
Other consumption includes housing consumption for owner-occupants, that is, the value of the annual services that home yields typically measured as the amount for which the home could be rented. The purchase of a home is a component of saving and investment. Consumer durables should be treated, in principle, in the same way as housing. Consumption is the value of the services from the durables. The purchase of the durable is then classified as saving. Household expenditure surveys typically report the rental value of owner occupied housing. Whether or not consumption of durables can be measured as a flow rather than a purchase will vary from country to country. If data on durable ownership are not available, the purchase of durables is treated as consumption.
The following items should be classified as transfers and not included in consumption: tax payments, gifts, remittances, donations, and similar items.
The following items are classified as asset-based reallocations and not included in consumption: the purchase of a home; the purchase of consumer durables, the purchase of stocks, bonds, and other securities; investment in a business or farm; increases in cash holdings; interest payments; rent on land. Expenditure surveys will vary in the extent to which these items are reported. Often saving is estimated as a residual, i.e., income plus net transfers less consumption.
Some items require particular attention although they may be unimportant in some countries or data may limit the extent to which they can be treated.
Insurance: Some insurance premiums (whole life insurance) are a form of saving. Consumers pay a premium and their policy accrues value that can be cashed in at a later date or borrowed against. This is saving. Other forms of insurance provide consumers with a way of pooling risk. Term life insurance and property and casualty insurance are examples of these forms of insurance. Some portion of premiums collected each year are paid to beneficiaries who have experienced the particular event being insured. These payments are transfers. Although they may produce inter-age reallocations, we assume that premiums are assessed in an actuarially fair way and, hence, produce only intra-age reallocations. Hence, they are not included in NTA. The remaining portion of premiums paid by consumers for the administrative costs and profits of insurance companies represents the cost and value of the risk-pooling services provided by insurance. It is classified as consumption by NIPA and by NTA.
The US NIPA has recently been revised because catastrophic losses, e.g., those produced by Hurricane Katrina, lead to large fluctuations in insurance related components. The new revisions measure the consumption of insurance services using an estimate of normal profits. Catastrophic losses that lead to actual profits that differ from normal profits are treated as a transfer.
Health: In NIPA private health consumption includes the value of all goods and services that are marketed, i.e., goods and services purchased from either private or public providers. Public health consumption includes only goods and services that are provided as in-kind transfers. Examples are the subsidized portion of public inoculation programs, public sanitation programs, free clinics, family planning programs, etc. Private consumption includes goods and services purchased and reimbursed through public cash transfer programs. Health consumption reimbursed by Medicare and Medicaid in the US and by National Health Insurance in Taiwan are classified as private health consumption in NIPA. However, in NTA, private health consumption that is reimbursed by the public sector is re-classified as public health consumption.
There are also important differences between NIPA and the NHA that should be kept in mind. First, NHA document expenditures rather than consumption. Expenditure is a broader measure that does not distinguish consumption from investment and profits. Private health expenditure, for example, includes the profits of insurance companies. Second, public national health expenditure in NHA includes both in-kind and cash transfers.
Separate procedures are used to allocate education, health, and housing and other consumption to household members. The methods described here are intended as illustrative and should be adapted to the particular circumstances of the country being analyzed and to the particular data that are available. The method of choice is to rely on individual level data for any consumption component, but these are rarely available.
Private Education Consumption
Education is typically allocated using a regression model. The household consumption of education (CFEj) is,
where is the number of enrolled members aged a (single age) in household j, and
is the number of not enrolled members aged a in household j. The number of members not enrolled captures educational spending that is not part of the formal educational system. Note that this equation is estimated in homogeneous form (without an intercept) insuring that household consumption is fully allocated.
The survey usually identifies who is enrolled and who is not in each household. If the information is not available, then each country team decides these age groups, based on the country’s schooling system. The age groups included varies with the country and with enrollment rates. In Taiwan, the number of enrolled includes those aged 3 to 29, although it varies by year.
The regression method may yield negative coefficients for some age groups with very low or no enrollments. If so, the negative coefficients should be replaced with zero to avoid negative expenditure.
The regression estimates are used to allocate the education expenditure for each household j to household member i. For example, for those who are enrolled:
where x is the age of the ith household member. Education consumption for those not enrolled is calculated in similar fashion. Stata programming code for Taiwan is available in the Appendix section.
Education consumption is intrinsically not smooth and the best approach is often to use the unsmoothed age profile to construct final estimates. Some smoothing at older ages may be warranted, however. Smoothing is discussed below.
Private Health Consumption
The allocation of private health consumption is difficult because of the complex ways in which it is financed. Three sources of finance are important in many countries: private out-of-pocket expense, private insurance, and the public sector. Different age allocation methods may be required for each of these components of health consumption.
National Health Accounts (NHA), available in some countries, provide a useful breakdown by source of finance.
The method used to allocate health varies depending on the availability of data.
Age profile of individual utilization measures. In some cases the expenditure survey may include utilization measures for household members. In this case, a model similar to the model employed for education can be used. For example, household health expenditure can be regressed on the number of members using outpatient services in each age group and the number of members using inpatient services in each age group. That is, the household consumption (CFHj) is regressed on the number of inpatients and outpatients aged a in each household:
Stata programming code for Taiwan is available in the Appendix section.
Age profile of utilization from alternative source. In some countries, such as Japan, per capita utilization by age is available from alternative sources. The household health consumption estimated is:
where U(a) represents a single utilization measure for each age, and Mj(a) is the number of household members aged a in household j. The estimated parameters are interpreted as the unit cost for each age. In some cases it may be reasonable to assume that the unit cost is independent of age, but this is probably an unattractive option for health services. Thus, the unit cost may be assumed to be quadratic in age, for example. In this case, the model to be estimated is:
As with the education method presented above, the estimated model is used to “predict” health expenditure for persons aged a. In this case, the predicted cost would be:
The predicted costs are used to allocate the observed health expenditure in each household to individual members. Then the health expenditures are tabulated to construct the per capita profile.
Iterative Method. This approach works by assigning health expenditure equally to each household member and then tabulating the per capita profile. The per capita profile is then used as weights to allocate health expenditure to household members producing a new per capita profile. The procedure can be repeated each time using the newly generated profile to allocate household expenditure. Under some conditions, this approach will converge to the actual underlying profile. Whether it will always do so is unknown at this point. An attractive feature of this method is that negative values will not be generated.
Simple Regression Approach. This approach is not recommended unless absolutely nothing else is possible. The regression approach used for health differs from the model used for education because there is no variable that capture which individuals are receiving health care services. Hence, household health expenditure is regressed on the number of household members in each age group
The age groups can be single year or broader age groups.
Private Other Household Consumption
All other household consumption is allocated to individuals using an ad hoc allocation rule based on an extensive review of the literature on household consumption. Evaluation of other methods, e.g., Engel’s method and the Rothbarth method, has shown them to be unreliable and we do not recommend that they be used.
Consumption of individuals living within any household j is assumed to be proportional to an equivalence scale that is equal to 1 for adults aged twenty or older, declines linearly from age 20 to 0.4 at age 4, and is constant at 0.4 for those age 4 or younger.
A formula for the scale is:
where D(x) is a dummy variable equal to 1 when condition x is met. Again, this scale is used to allocate the expenditure for each household j to household member i.
where x is the age of the ith household member. Stata programming code for Taiwan is available in the Appendix section.